If you want to know when adherence breaks, don’t look at refill data. That’s the autopsy. The early signals show up weeks earlier—in the questions patients ask when something starts to feel “off.”
Read enough of them, and a pattern emerges. Not dramatic. Not explicit. But consistent.
1) “Can I mix this with…” → the interaction anxiety phase
This isn’t curiosity. It’s risk calibration. Patients are probing for hidden dangers—and when answers feel uncertain, discontinuation becomes the simplest “safe” option.
2) “Are these side effects normal?” → the doubt phase
Notice the framing: not “I’m stopping,” but “is this expected?” They’re looking for reassurance. If they don’t get it, they start experimenting—skipping doses, spacing them out.
At this point, adherence is hanging by a thread. Any friction—price, access, complexity—tips it.
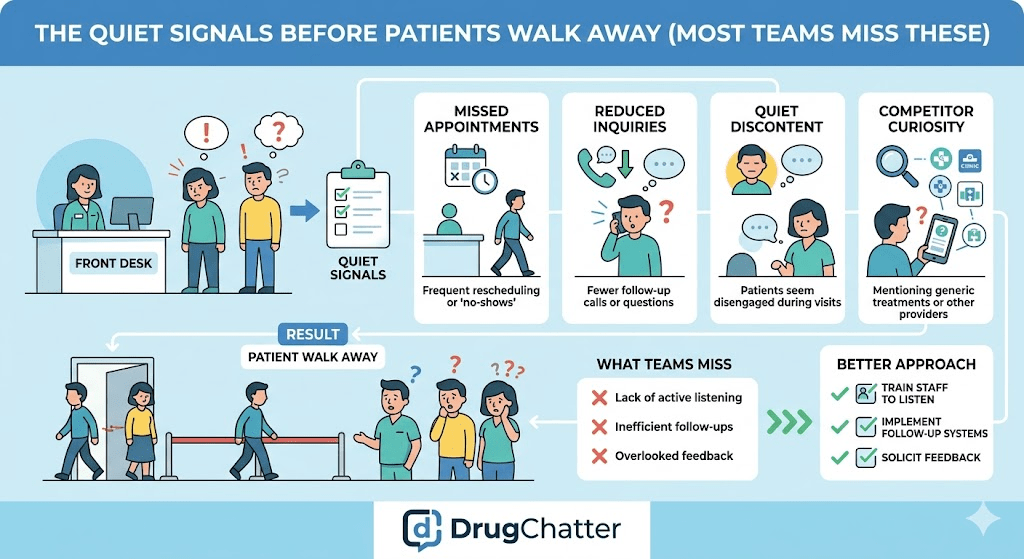
What this means (and what most teams miss)
No one wakes up and decides to stop therapy. They drift there—through uncertainty, unmanaged side effects, self-adjustment, and fading belief in benefit.
The key insight: Adherence drop-off is not a single event. It’s a sequence of questions.
And those questions are visible—early—if you’re looking in the right place.
Ignore them, and you measure churn after it happens. Track them, and you can intervene before the patient ever leaves.